


Why Three Doctors are in Favor of Decentralized Clinical Trials
Talk to us about implementing digital-first health solutions.
Want to learn more about implementing digital-first health solutions?

The Pandemic Enters, Stage Left
The 2020 global SARS-CoV-2 pandemic accelerated political, regulatory, and public acceptance of the role of digital therapeutics in providing high quality medical care. Most evidently, the near halt of ongoing traditional clinical trials highlighted the critical need for creative, progressive research designs that offer patients access to therapeutics for life-threatening and chronic diseases.
Dr. Pamela Diamond recounted to The Sidebar:
Starting up CURAVIT Clinical Research during the COVID-19 pandemic presented many challenges, but, in a lot of ways, the pandemic accelerated the growth of our company. There were many site-based trials that came to a screeching halt in early 2020. Participants could not get into the sites for their assessments. In many ways, the challenges of the pandemic made sponsors, research groups, CROs (contract research organizations), and participants more open-minded about becoming involved in Decentralized Clinical Trials.
Intuitively, DCTs are patient centric. However, while acknowledging the benefits of trial modifications, regulatory agencies and industry stakeholders strive to provide evidence of DCT efficacy, both clinically and economically.
What’s the Evidence Supporting DCTs?
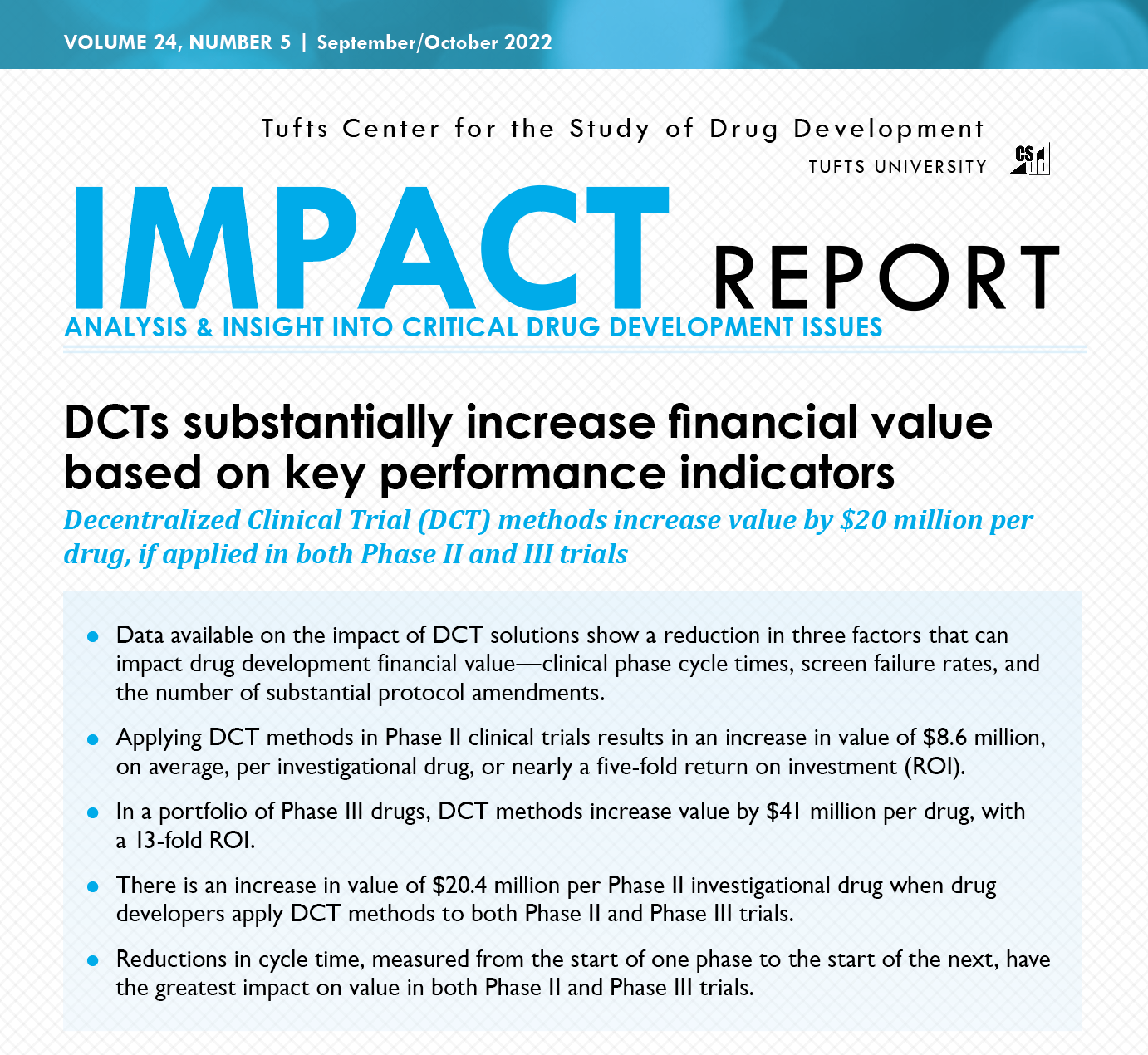
A 2022 Tufts Center for the Study of Drug Development (CSDD) Impact Analysis showed that using DCT methods in Phase II studies provided a five-fold ($8.6 million) return on investment (ROI), and a 13x ROI for Phase III drugs ($40.1 million dollars) per investigational drug. This was based on an independent analysis of DCTs from Medable.
Tufts CSDD analysis concluded that the largest benefit results from reductions in cycle time moving from Phase II to Phase III clinical trials.
Analyzing industry confidence in DCTs, McKinsey & Company reported that in 2020, 100% of pharma and CRO participants surveyed responded they expected virtual trials to be a major component of their portfolios. And 89% anticipate their company running home-based clinical trials with participants—representing a dramatic increase in endorsement of DCTs from 2019.
Are Regulatory Agencies ‘On Board’?
Regulatory agencies recognize that traditional clinical trials are expensive. In a 2018 study, Johns Hopkins researchers identified that clinical trial costs can range from $2 million dollars to $347 million dollars. The number of participants, length of the trial, and the ability to meaningfully influence clinical outcomes of the targeted disease can increase costs significantly.
In 2007, the FDA proposed the Clinical Trials Transformation Initiative, but it wasn't until 2011 that Pfizer implemented the first virtual DCT, according to Dr. Gail A. Van Norman in Decentralized Clinical Trials: The Future of Medical Product Development?
The Sidebar asked Dr. Michelle Longmire, CEO of Medable, why the medical research and pharma communities were slow in embracing DCTs—until now. Dr. Longmire explains:
The stakes are high. You have patients’ lives on the line, and an expensive process, close to 3 billion dollars, according to Tufts. I think that it’s hard for people to deviate from the status quo unless they must.
We didn’t get meaningful adoption of DCTs until the pandemic, when we actually had to get people to do it differently because the sites were closed. The status quo is all that people are willing to go with until there is something that forces them to change.
In a 2021 meeting of the directors for NCI-designated cancer centers, FDA regulators demonstrated enthusiasm and embracement of DCTs. In addition to predictable benefits like improved recruitment, they identified these benefits of DCTs:
• Data capture outside of the healthcare setting.
• Continuous data rather than snapshots.
• Objective measurements.
• Reduced missing data.
• Capturing rare events.
Recognizing the advancement of DCTs, the FDA’s Oncology Center of Excellence is now evaluating how modifications made to oncology clinical trials, during the COVID-19 pandemic, can be assessed for quality of evidence and future trial guidance.
The Sidebar queried Dr. Pamela Diamond, Chief Medical Officer of CURAVIT, on her experience regarding the FDAs’ uptake of DCTs. She noted:
An impetus was the COVID-19 response. In late 2021 and early 2022, the FDA published guidelines on DCTs: services and on the use of digital health products in trials. Those guidelines have been very helpful.
I think it is good advice to sponsors, CROs–anyone designing and executing DCTs–to consult the FDA early and often. It’s helpful to get the input of the FDA about the protocol design and product-specific questions, garnering the FDAs advice on the selection of technology that might be used in conducting the research trial.
Are the Central Stakeholders Ready to Pivot?
DCTs can’t progress without their two main stakeholders embracing the transition: patients and clinician-researchers. In 2021, Labcorp™sponsored a survey of US and UK oncology clinician researchers’ and patients’ perceptions of DCTs. The by oncologists revealed they were reticent about possible decreased oversight, increased patient responsibility, and quality of samples.
Patients, on the other hand, revealed their general concerns were related to the potential for side effects to occur, distance from the hospital, or not receiving the therapeutic drug (receiving a placebo). Confirming The Sidebar’s observations, of the patients surveyed, 90% revealed they would not travel over 10 to 50 miles to participate in a research study.
Regarding exclusions to patient participation in research, Dr. Ray Dorsey, Professor of Medicine at the University of Rochester recounts his philosophy:
We have cared for patients in 5 states, and 6 continents. Since 2007, we have performed at least a dozen decentralized studies involving thousands of individuals with and without Parkinson’s disease and other conditions over the last ten years.
Dr. Dorsey concludes:

How do we do that? We don’t do that by embracing the status quo. We do that by developing new approaches that leverage technology to bring care to patients and research opportunities to participants. When we do that, we get a more equitable system, better health, and better knowledge that can fuel better treatments!
DCTs: Broadening Access, Enhancing Equity
Clinician-researchers and patient advocacy groups recognize the challenges and limitations of traditional clinical trials, which has inadvertently excluded patients in diverse socioeconomic and cultural strata. The onset of the COVID-19 pandemic pushed industry stakeholders, researchers, and patients to view clinical trial participation in a new light.
These broadened perspectives are buoyed by increased clinician support and patient acceptance for digital therapeutics' role in supporting healthcare and DCTs. With increasingly creative DCT designs, even patients with limited digital access have the opportunity to participate in emerging treatments. DCTs are now ‘center stage’ in effecting clinical trials—facilitating rapid progress in crucial drug development, enhancing diversity and interpretability of trial results, and enhancing equity in patient access.
In Part II of our series, Natural Allies: Decentralized Clinical Trials and Digital Therapeutics, we will explore how DTx and DCTs are inter-reliant, augmenting patient participation in the worlds’ best investigational solutions.
About the author
.jpg)
Mary McGorray, MD
Mary McGorray is a medical writer and board-certified internist who writes about medical innovation, healthcare economics, and public policy.





.png)


.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)

.jpg)
.jpg)

.jpg)




.png)

.jpg)
.jpg)
.jpg)



%201%20(1).jpg)
.jpg)
.jpg)

.jpg)
%201%20(1).jpg)
.jpg)


%201%20(1).jpg)



.jpg)

.jpg)


.png)
.jpg)
.jpg)
%201%20(1).jpg)

%201%20(1).jpg)
%201%20(1)%20(1).jpg)
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)
.jpg)

.jpg)
%201%20(1).jpg)


.jpg)

.jpg)
.jpg)
%201%20(1)%201%20(1).jpg)

.jpg)
.jpg)

.jpg)

.jpg)

.jpg)
.jpg)

%201%20(1).jpg)
.jpg)

.jpg)
.jpg)
.png)

.png)
.jpg)


.jpg)
.png)
.jpg)
{kind=link}
{kind=link}